
Drug and alcohol rehabilitation centers address patterns of problematic substance use through organized programs that match levels of clinical care to individual needs. These centers commonly categorize services by intensity and duration, ranging from medically supervised detoxification to structured residential programs and less-intensive outpatient supports. Facilities may operate within hospitals, standalone treatment centers, or community clinics, and many refer to nationally recognized frameworks such as the American Society of Addiction Medicine (ASAM) criteria when determining appropriate care levels.
Programs at these centers typically include clinical assessment, behavioral therapies, and coordination with primary care or mental health providers as needed. Teams often involve clinicians, counselors, nursing staff, and peer-support specialists who document progress and adjust care plans over time. In the United States, regulatory and payor environments — including state Medicaid policies and private insurance provisions — shape which services are available and how they are delivered, so models can vary geographically and by facility type.
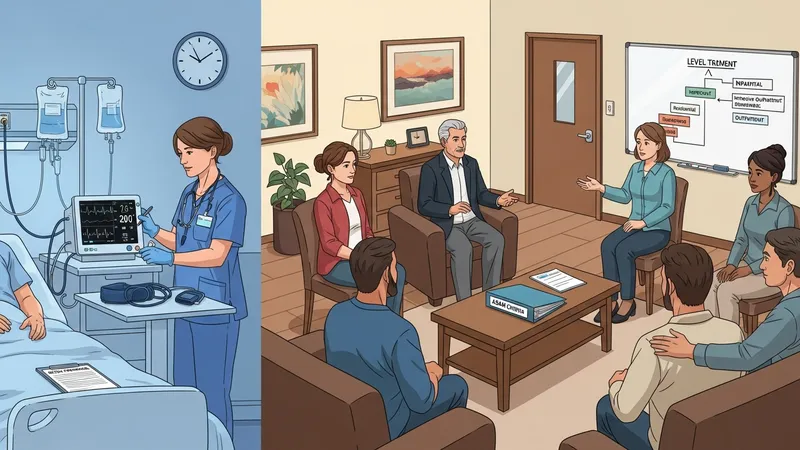
Levels of care are frequently defined by intensity and service mix rather than uniform labels, and a person’s placement often follows a clinical assessment. The ASAM criteria is one U.S.-based system that categorizes needs across dimensions such as withdrawal potential, medical conditions, and readiness to change; many U.S. programs reference it when determining whether a person may need outpatient care, residential treatment, partial hospitalization, or medically managed inpatient services. This approach aims to match resources to clinical indicators and social supports.
Detoxification or medically supervised withdrawal services may be a first step for some individuals who require management of acute physiological symptoms. Such services often occur in specialized units or hospitals and may be short-term. Clinical teams typically assess withdrawal risk and may coordinate medication and monitoring when appropriate. Detox alone is usually framed as an initial stabilization phase rather than a complete treatment plan, and transition to psychosocial or ongoing care is commonly part of discharge planning.
Behavioral therapies are core components across care levels and can include individual cognitive-behavioral therapy (CBT), motivational interviewing (MI), family therapy, and group modalities. In the U.S., evidence-informed therapies are often integrated with medication when clinically indicated. Programs may vary in how routinely they use particular therapies and in staff training; consumers and referring clinicians may review program descriptions and clinical credentials to understand which therapeutic approaches are emphasized.
Care coordination and discharge planning often aim to link people to continuing supports such as outpatient counseling, peer recovery groups, and community resources. In the United States, partnerships with primary care, mental health services, and social services can influence continuity of care. Confidentiality rules and documentation standards are part of program operations, and facilities commonly have protocols for referrals, follow-up appointments, and communication across providers to support ongoing engagement.
In summary, centers that treat drug and alcohol problems operate across a spectrum of care levels and service types intended to address stabilization, clinical therapy, and long-term recovery support. Programs may use standardized assessment frameworks to guide placement and often combine behavioral therapies with medical management when indicated. The next sections examine practical components and considerations in more detail.
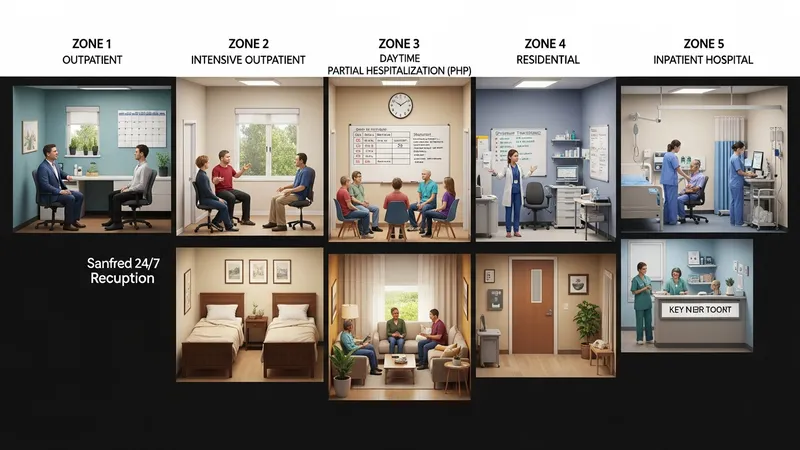
Care levels commonly range from early intervention and outpatient counseling to intensive residential or inpatient services. In the United States, many facilities classify services as outpatient, intensive outpatient (IOP), partial hospitalization (PHP), residential, and inpatient hospital care. Each level typically differs by hours of clinical contact, 24-hour availability, and the degree of medical oversight. Facilities frequently describe the scope of services they provide and whether they follow ASAM placement criteria, which helps clinicians and families compare how a center defines intensity and transition points.
Facility examples in the U.S. illustrate these distinctions: outpatient programs may provide weekly individual therapy and group sessions, IOPs often offer multiple hours per day several days per week, and residential programs provide round‑the‑clock supervision. National directories and state licensing databases commonly list the types of licensure and services available at each center. When reviewing options, it may be helpful to note the typical daily schedule and staff roles associated with each care level to understand how intensity translates into services delivered.
Many centers describe integration of medical evaluation and psychiatric assessment as part of initial placement. For people with co-occurring mental health conditions, combined behavioral health services may be offered on-site or via formal referral agreements. The presence of credentialed medical personnel or formal partnerships with hospitals can influence whether a facility provides medically managed detoxification or refers out to hospital settings when higher levels of medical care are required.
Data sources such as the Substance Abuse and Mental Health Services Administration (SAMHSA) and state health departments provide listings and program descriptions that reflect observed patterns across the U.S. These resources may show that program availability and commonly used care models differ by region; rural areas, for example, often rely more on outpatient and telehealth services whereas urban regions may have greater access to residential beds. Such patterns inform how systems plan and allocate resources.
Clinical offerings in U.S. programs often include a mix of psychotherapy, group interventions, family services, and case management. Behavioral therapies commonly used include cognitive-behavioral therapy (CBT), contingency management, and motivational enhancement approaches; many programs tailor therapy intensity to individual needs and the chosen care level. Research summaries from U.S. agencies such as the National Institute on Drug Abuse (NIDA) describe these modalities and note that combining behavioral therapy with appropriate medication management can be a component of comprehensive care for certain substance use disorders.

Medication-assisted treatment (MAT) for opioid and, in some cases, alcohol use disorders is available in many U.S. outpatient and clinic settings and may be incorporated into residential programs where permitted. MAT typically involves FDA-approved medications plus counseling and support. Regulatory frameworks, state prescribing guidelines, and availability of waivered clinicians (for some medications) shape how MAT is delivered across different jurisdictions in the United States.
Peer support and recovery-oriented services often complement clinical interventions. In the U.S., peer recovery specialists may be employed by treatment centers or community organizations to provide lived-experience support, linkage to community recovery resources, and assistance with navigation of social services. These roles are usually described as adjunctive supports that can supplement clinical care rather than replace professional treatment.
Outcome measurement varies across programs; some centers use standardized tools for symptom tracking and functional assessments, while others report on service engagement metrics such as attendance and completion rates. National initiatives and state reporting systems in the U.S. encourage collection of consistent indicators to inform program planning, but methods and frequency of measurement can differ by provider and funding source. Considering how a program monitors progress may help stakeholders understand its clinical orientation.
Payment and access considerations are significant in the U.S. landscape. Coverage policies vary: many state Medicaid programs reimburse a range of substance use disorder services, private insurance plans often cover medically necessary treatment under parity laws, and Medicare covers certain services for eligible beneficiaries. Facility billing practices and prior authorization requirements can influence how quickly a person can begin a specific level of care. SAMHSA and state Medicaid web pages provide guidance on program eligibility and typical coverage categories.

Costs for residential or specialty services can vary widely depending on licensure, facility ownership, and the mix of services provided. Publicly funded and nonprofit programs may offer sliding-fee scales or accept Medicaid, while private facilities typically charge different rates and may rely on private insurance reimbursements. Rather than assuming uniform pricing, it can be informative to review a center’s stated billing policies and the range of payors they accept within the specific U.S. state or county where the facility operates.
Geographic distribution affects access: metropolitan areas in many states often have a greater number of licensed residential beds and outpatient providers, while some rural counties may have limited in‑person services and rely on telehealth or regional referral networks. State behavioral health agencies often publish provider directories and mapping tools to show service availability. These patterns influence wait times and transportation needs, which are practical considerations for service planning.
Administrative considerations such as documentation requirements, confidentiality under federal rules (including 42 CFR Part 2 for substance use treatment records), and state licensure standards shape how centers operate and share information. Understanding these regulatory aspects in the relevant U.S. jurisdiction may clarify what information will be requested during intake and how care coordination is managed across providers and systems.
Continuing care after an initial episode is commonly framed as part of comprehensive service design in the United States. Many centers outline transitional plans that link people to outpatient therapy, peer recovery groups, community-based supports, or medication follow-up. Research summaries from U.S. agencies suggest that ongoing engagement with recovery-oriented services often supports sustained participation in care; descriptions frequently note associations rather than causal guarantees and emphasize individualized planning for maintenance and relapse prevention.

Programs may use a variety of tools to track outcomes, including standardized screening measures, attendance records, substance use self-reports, and referrals completed. State reporting systems and grant-funded initiatives often require collection of specific metrics to evaluate service utilization and program performance. These data help policymakers and administrators identify service gaps, plan capacity, and inform quality improvement efforts within the U.S. treatment system.
Peer-based continuing supports such as recovery community organizations and mutual‑help groups are common components of post‑treatment planning in many U.S. localities. Centers often describe partnerships or referral pathways to these community resources. While the role and availability of peer supports vary regionally, they are typically presented as one element among several that individuals may consider when designing a longer-term support network.
When reviewing program outcome information, it is useful to note how measures are defined and over what time frames results are reported. Programs and evaluators in the United States may report short-term engagement metrics separately from longer-term functional or quality-of-life indicators. Clear definitions and consistent measurement approaches can aid interpretation of reported outcomes and support comparisons across service models without implying guaranteed results.