
Orthopedic surgery is the medical specialty that addresses conditions affecting the musculoskeletal system, including bones, joints, ligaments, tendons, muscles, and nerves. The field encompasses a range of procedural approaches intended to restore function, reduce pain, or stabilize structures after injury or disease. Common procedural categories include joint-preserving techniques, joint replacement, minimally invasive arthroscopy, and fixation of fractures; each category involves distinct diagnostic steps, operative methods, and recovery pathways. Discussion of these areas typically emphasizes clinical assessment, imaging, and multidisciplinary planning rather than predicting individual outcomes.
Care pathways in orthopedic surgery describe the sequence of clinical steps that guide a patient from initial assessment through recovery and follow-up. These pathways often integrate preoperative evaluation, perioperative management, standardized operative protocols, and staged rehabilitation plans. Elements such as comorbidity assessment, imaging review, and coordination with physical therapy services commonly shape pathway design. Pathways may vary by procedure type, institution, and regional practice patterns, and they frequently aim to align clinical resources with measured recovery milestones while remaining adaptable to patient-specific factors.
Preoperative planning for orthopedic procedures often includes a structured assessment that may involve medical clearance, imaging, and functional evaluation. Imaging modalities such as X-ray, CT, or MRI typically inform surgical approach and implant selection, while history and physical examination help identify comorbid conditions that can affect perioperative risk. Preoperative pathways may also incorporate patient education about expected recovery phases and coordination with allied services like physiotherapy and occupational therapy. These preparatory steps are commonly used to align expectations and to reduce variability in perioperative management.
Operative techniques in orthopedics vary widely by anatomical site and intended goal; for example, arthroscopy often focuses on visualization and repair through small portals, whereas arthroplasty involves component alignment and fixation. Surgical teams frequently balance considerations such as tissue handling, implant biomechanics, and blood management when selecting intraoperative strategies. In many settings, standardized checklists and team briefings are used to coordinate roles and equipment needs. Technique selection typically reflects a combination of pathology, surgeon training, and available technology rather than a single universal approach.
Postoperative care pathways commonly include staged rehabilitation plans that progress from protected mobilization to strength and functional training. Early goals often emphasize safe mobilization, pain control using multimodal strategies, and prevention of complications such as wound issues or thromboembolic events. Rehabilitation timelines may vary by procedure; for instance, recovery phases for joint replacement can differ in duration from those for complex fracture fixation. Coordination between surgical teams, rehabilitation professionals, and primary care clinicians often supports continuity of care across these phases.
Multidisciplinary coordination is a central component of many orthopedic care pathways and may involve surgeons, anesthesiologists, nurses, physiotherapists, and case managers. Communication across disciplines can support tailored perioperative plans, particularly for patients with multiple health conditions. Pathway adaptations often occur in response to patient progress, laboratory results, or imaging findings, and ongoing reassessment helps guide decisions about weight-bearing status, activity progression, and timing of follow-up assessments. Such coordination typically aims to match clinical resources to patient needs without prescribing a single standardized regimen.
In summary, orthopedic surgery and its associated care pathways encompass a continuum from detailed preoperative assessment through operative technique selection and staged rehabilitation. Common procedural examples include joint replacement, arthroscopy, and fracture fixation, each with distinct planning and recovery considerations. Pathways often combine standardized elements with individualized adjustments based on patient factors and clinical findings. The next sections examine practical components and considerations in more detail.
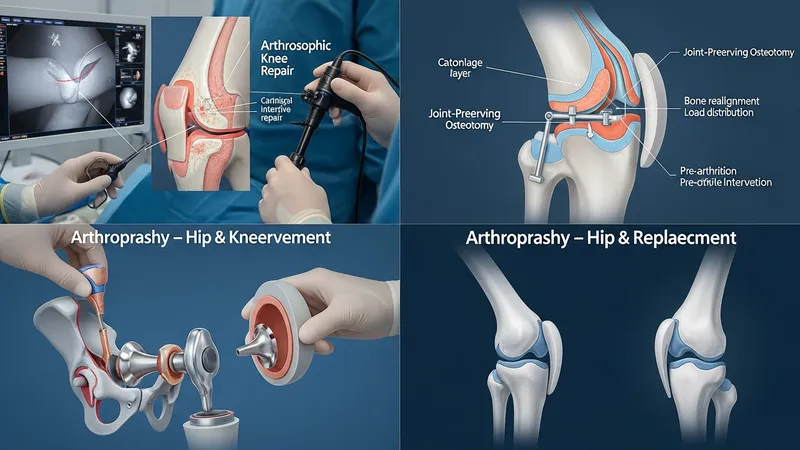
Procedural selection in orthopedic practice generally follows anatomic diagnosis, symptom burden, and functional limitation. Joint-preserving procedures such as osteotomy or cartilage repair may be considered when degenerative changes are limited and the goal is to maintain native joint structures. Joint replacement (arthroplasty) is often considered when articular surfaces are extensively compromised and pain or function is substantially affected. Fracture fixation choices depend on fracture classification, bone quality, and soft-tissue status, with options ranging from internal plates and screws to intramedullary nails and external fixators. Indication patterns may vary by age, activity level, and comorbidity profile.
Minimally invasive arthroscopic techniques are frequently applied to intra-articular pathology because they can allow targeted repair through small incisions and may reduce soft-tissue disruption. These methods often address meniscal tears, ligament injuries, or chondral lesions using specialized instruments and suture-based repairs. Conversely, open procedures remain necessary for extensive reconstructions, complex fracture patterns, or when direct exposure is required for stable fixation. Decision-making commonly weighs the anticipated tissue environment, repair durability, and rehabilitation implications rather than assuming one approach fits all cases.
Implant and fixation technology choices can substantially influence operative planning and postoperative management. Implant options include cemented versus cementless components in arthroplasty, modular designs for complex reconstructions, and a variety of plate and nail systems for fractures. Material properties, biomechanical fit, and surgeon familiarity typically inform selection. In many clinical settings, implant registries or institutional protocols may provide comparative data on performance patterns, which can help practitioners align device choices with expected operative scenarios while acknowledging that outcomes depend on multiple interacting factors.
Indication thresholds and timing for surgery also reflect broader care pathway goals, including optimization of health status before intervention. For elective procedures, preoperative optimization of nutritional status, glycemic control, or cardiovascular risk factors may be integrated into the pathway to reduce perioperative variability. For acute injuries, timing decisions often balance the need for early stabilization with the requirement to address soft-tissue concerns. These considerations typically aim to create a predictable operative environment and a structured rehabilitation trajectory.
Preoperative planning commonly begins with a comprehensive clinical assessment and targeted imaging to characterise pathology and guide surgical approach. Plain radiographs are often first-line for bony alignment and joint space assessment, while CT or MRI may provide more detailed views of complex fractures or soft-tissue lesions. Laboratory tests and medical consultation may be used to identify comorbid conditions that can influence anesthesia or wound healing. In many practices, standardized preoperative checklists and pathway documents are used to ensure essential steps—such as medication reconciliation and risk stratification—are completed before operation.
Patient education and expectation alignment are frequently part of preoperative pathways and may include discussion of typical recovery timelines, potential complications, and rehabilitation goals. Education tools can be verbal, written, or multimedia and often cover mobility restrictions, weight-bearing status, and signs that warrant clinical review. These informational elements typically aim to support adherence to postoperative protocols and to help patients and families plan for home support during early recovery phases. Education is usually framed as informative rather than prescriptive, acknowledging individual variability in recovery.
Optimization of modifiable risk factors is a common component of preoperative care and may include management of anemia, smoking cessation strategies, and assessment of nutritional status. These efforts often occur in collaboration with primary care or specialty services and are intended to reduce perioperative complications rather than to guarantee specific outcomes. For patients with significant medical comorbidities, multidisciplinary case reviews or preoperative anesthesia consultations may be employed to tailor perioperative monitoring and perioperative medication plans.
Pathway scheduling and resource coordination are practical considerations within preoperative planning that can influence patient flow and postoperative recovery. Prehabilitation programs may be offered in some settings to improve baseline strength and mobility prior to surgery, and scheduling processes often coordinate operative timing with availability of rehabilitation services. Such operational elements typically aim to smooth transitions between stages of care and to align clinical capacity with patient needs, while allowing adjustments based on individual clinical factors.
Intraoperative decision-making commonly addresses anesthesia type, positioning, and approach selection as foundational elements of operative technique. Regional anesthesia techniques may be used alone or in combination with general anesthesia depending on patient factors and procedure type, and positioning is selected to optimise exposure while preserving neurovascular safety. Surgical exposure and soft-tissue handling practices typically prioritise preservation of critical structures and containment of bleeding. Use of intraoperative imaging, such as fluoroscopy, can assist in implant placement and fracture reduction for improved procedural accuracy.

Implant handling and fixation strategies are central to many orthopedic operations and may involve temporary fixation, definitive hardware placement, and intraoperative testing of stability and range of motion. For arthroplasty, component alignment and soft-tissue balancing are often steps that influence early function; for fracture fixation, restoration of anatomic alignment and stable construct selection guide weight-bearing recommendations. Surgeons commonly weigh trade-offs between rigid fixation for early mobilization and biological considerations that support bone healing when choosing constructs.
Blood management and infection prevention are consistent intraoperative considerations across procedure types. Strategies may include meticulous hemostasis, use of topical agents, and protocolized antibiotic administration timed appropriately to incision. Sterile technique, instrument handling, and wound closure methods are part of broader infection control practices. In many settings, surgical teams follow institutional protocols designed to reduce variability and to document intraoperative steps that may impact postoperative monitoring and rehabilitation.
Technology integration, such as navigation systems or robotic assistance, is increasingly available for select orthopedic procedures and may be used to enhance alignment or reproducibility of component placement. The adoption of such tools often depends on institutional resources, surgeon training, and case selection. When used, these technologies typically supplement, rather than replace, standard surgical principles and clinical judgement. Teams generally consider the incremental benefits of technology against workflow implications and training requirements.
Immediate postoperative care typically focuses on monitoring vital signs, assessing wound status, and initiating early mobilization when appropriate. Pain management strategies often use multimodal approaches to reduce reliance on any single medication class, and protocols for thromboprophylaxis or antibiotic continuation are usually aligned with procedural risk profiles. Early physical therapy interventions may begin in the acute setting to promote safe transfers and joint range of motion, with progression tailored to the procedure and the stability of surgical constructs.

Rehabilitation is generally organised into phases that move from protected activity and swelling control to progressive strengthening and functional retraining. Phase durations often vary: an uncomplicated arthroscopic repair may progress more quickly to resisted activity than a major reconstructive procedure, which can require prolonged supervised therapy. Rehabilitation plans typically consider patient-specific factors such as baseline mobility, comorbidities, and social supports, and are adjusted based on clinical milestones and healing assessments rather than fixed timelines.
Follow-up and monitoring are routine elements of postoperative pathways and may include scheduled clinic visits, repeat imaging, and functional assessments. Follow-up intervals are often determined by the procedure type and the expected healing course; for example, fracture fixation may require earlier imaging to confirm alignment, while arthroplasty follow-up often emphasises functional outcomes over longer intervals. Monitoring for complications such as wound problems, implant-related issues, or delayed healing typically follows established clinical signs rather than predictive guarantees.
Coordination with allied health professionals is a key consideration for longer-term recovery and return to activity. Occupational therapy, community rehabilitation services, and primary care clinicians can all contribute to continuity of care after discharge. Pathways that include clear communication about weight-bearing status, activity modifications, and criteria for escalation of care are commonly used to support safe recovery. These coordinated approaches aim to integrate clinical judgment with structured rehabilitation without implying specific outcomes for any individual patient.