
Cosmetic and plastic surgery refers to a set of surgical and non-surgical procedures aimed at restoring form or altering appearance for functional or aesthetic reasons. Plastic surgery commonly includes reconstruction after trauma, congenital differences, or disease, while cosmetic procedures typically focus on modifying features to meet patient aesthetic preferences. Both areas overlap in technique, perioperative planning, and outcome assessment; surgeons may perform similar operative steps but with differing primary goals. Discussion of common procedures involves understanding procedural intent, typical timelines, and the clinical frameworks used to evaluate risks and benefits without implying specific outcomes for any individual.
Practices in this field often combine preoperative assessment, intraoperative technique, and postoperative care into coherent pathways that clinicians use to manage patients. Preoperative imaging, consultation about expectations, and assessment of medical suitability may be part of routine planning. Intraoperative choices—such as incision location, tissue handling, and use of implants or grafts—can influence healing trajectories. Follow-up care typically includes wound checks, activity guidance, and monitoring for complications. Descriptions below outline representative procedure categories and the considerations commonly associated with each, framed as informational examples rather than prescriptive advice.

Comparing these categories highlights differences in objectives and typical clinical workflows. Reconstructive procedures often prioritise functional restoration and may be staged over multiple operations, whereas cosmetic procedures commonly prioritise appearance and may be scheduled electively. Many procedures blend aims: for example, breast reconstruction after cancer combines oncologic considerations with aesthetic planning. Recovery patterns can vary by procedure type; some interventions involve short recovery phases measured in days, while others may require weeks to months for tissue remodelling. Outcome measurement frequently uses photographic documentation, patient-reported measures, and objective scales to track progress over time.
Risk assessment and informed discussion are central to decision-making across these examples. Clinicians typically evaluate medical history, comorbid conditions, and realistic expectations before recommending a surgical plan. Preoperative optimization—such as managing chronic illnesses, adjusting medications, and tobacco cessation where relevant—may be advised by providers as part of preparation. The informed discussion commonly includes potential complications that can occur with any invasive procedure, general timelines for healing, and the range of possible interventions for problems that may arise. These are presented as considerations rather than guarantees of outcome.
Technique selection and procedural staging often reflect anatomical variables and patient-specific goals. For instance, implant-based breast procedures may use different pocket planes or implant types depending on tissue characteristics, while flap-based reconstruction relies on vascular anatomy and donor-site considerations. Facial procedures depend on regional anatomy and the relative position of soft tissues and bony structures. Body contouring approaches vary with skin elasticity and distribution of adipose tissue. Surgeons often describe multiple technical options and may plan procedures to balance aesthetic aims with preservation of function and tissue viability.
Outcome evaluation generally combines clinician assessment with patient-reported outcomes and standardized scales where available. Assessment may include measurements of symmetry, scar appearance, sensory changes, and functional metrics such as range of motion or breathing function when relevant. Clinicians often schedule serial follow-ups to monitor wound healing and to identify complications early. Rehabilitation, scar management, and secondary revisions can be part of long-term care planning. These practices may vary by procedure type and clinical setting, and they typically aim to provide structured monitoring rather than guaranteed results.
In summary, cosmetic and plastic surgery encompasses a range of procedures—breast, facial, body contouring, and reconstructive interventions—that share common planning, technical, and follow-up frameworks. Each category presents distinct anatomic and functional considerations, and clinicians typically frame expected recovery and risks in probabilistic terms. The next sections examine practical components and considerations in more detail, including types of procedures, preoperative assessment, intraoperative technique, and postoperative care.
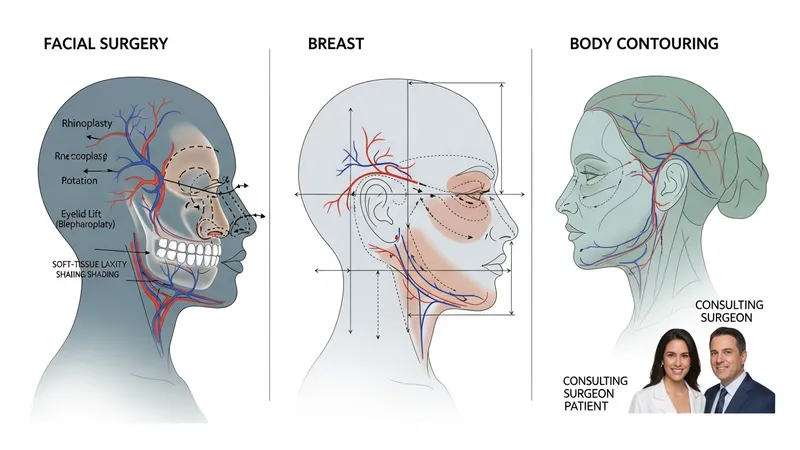
Procedure categories in cosmetic and plastic surgery can be described by anatomical region and by primary goal, such as reconstruction versus aesthetic alteration. Facial procedures may address nasal structure, eyelid position, or soft-tissue laxity, and they often require detailed analysis of facial proportions and skin quality. Breast-related procedures may focus on volume modification, reduction, or reconstruction after tumor removal, each with different technical approaches. Body contouring addresses adipose distribution and redundant skin, frequently following weight loss. Reconstructive cases commonly use grafts or flaps to restore tissue continuity and function. These categories provide a framework for clinicians to select operative strategies aligned with patient-specific factors.
Within each category, technique selection often reflects trade-offs between invasiveness, expected recovery, and potential need for revision. Less invasive options may involve local excisions or office-based procedures with shorter recovery, while complex reconstructions can be staged and require longer convalescence. Scar placement, tissue tension, and vascular supply are technical variables that may influence immediate intraoperative decisions and long-term appearance. Clinicians typically discuss multiple technical options and explain how each may affect healing timelines and secondary procedures, using descriptive comparisons rather than prescriptive recommendations.
Typical applications of these procedure categories vary by patient needs and clinical indications. For example, breast reconstruction following oncologic surgery may prioritise restoration of chest wall contour and symmetry, whereas cosmetic breast modification commonly addresses volume and proportion. Facial procedures can address both function and appearance, such as rhinoplasty for breathing and nasal form. Reconstructive strategies for trauma often require multidisciplinary coordination, including orthopaedics or neurosurgery when deeper structures are involved. Framing procedures by application helps set realistic expectations about stages of care and follow-up requirements.
When considering procedural categories, clinicians frequently reference outcome measures that are relevant to each type. These may include validated patient-reported outcome instruments for breast surgery or scar assessment scales for cutaneous procedures. Objective measures—such as symmetry indices, range-of-motion testing, or photographic comparison—can supplement subjective reports. Such metrics are used to guide follow-up care and to inform decisions about potential secondary procedures, and they tend to be applied as evaluative tools rather than as predictors of individual results.
Preoperative planning commonly includes a detailed medical history, focused physical examination, and discussion of patient goals and expectations. Clinicians may use standardized forms or visual aids to document baseline status and to explore what outcomes the patient seeks. Medical suitability assessments often include review of comorbid conditions, medication use, and factors affecting wound healing. In many settings, imaging or photographs are taken for documentation and surgical planning. The planning phase may also address anesthesia options and perioperative risk mitigation strategies, presented as considerations rather than prescriptions.

Informed consent is a central element of preoperative assessment and typically covers procedural steps, common risks, alternative approaches, and follow-up requirements. Discussions about potential complications often use probabilistic language to convey uncertainty, emphasising that individual recovery can vary. Some clinicians incorporate validated decision aids or patient-reported outcome questionnaires to clarify expectations. Psychological readiness and social support considerations may also be part of assessment, particularly for elective cosmetic procedures where expectations and coping with recovery can affect satisfaction and adherence to postoperative instructions.
Timelines for preoperative preparation can vary by procedure complexity. Simple office-based procedures may require minimal preoperative testing, while major reconstructive operations might involve laboratory tests, imaging, or specialist consultations. Smoking cessation, optimization of chronic conditions (such as diabetes or hypertension), and guidance on medications that affect bleeding are commonly discussed as preparatory steps that may influence surgical risk. These preparatory measures are typically framed as strategies to reduce risk or support healing rather than guarantees of specific outcomes.
Planning often incorporates multidisciplinary input when indicated. For example, breast reconstruction after oncologic surgery may involve coordination with oncology teams, while complex facial reconstruction may include maxillofacial or ENT specialists. Multidisciplinary planning can facilitate staging of procedures, timing relative to other treatments, and rehabilitation needs. Such coordination is described as a logistical and clinical consideration that may affect scheduling and resource allocation rather than an assurance of a particular result.
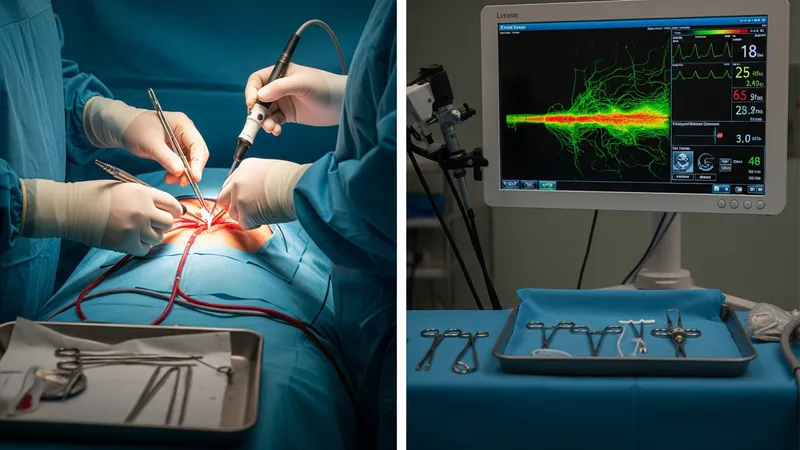
Operative technique selection is influenced by anatomy, tissue quality, and the procedural goal—reconstructive or aesthetic. Surgeons may choose between open, endoscopic, or percutaneous approaches depending on access needs and desired contouring. Tissue handling, preservation of vascular supply, and decisions about implants versus autologous tissue are technical factors that can influence healing and appearance. Intraoperative monitoring of bleeding, perfusion, and tissue viability is routinely used to guide immediate decisions. These intraoperative considerations are presented as typical clinical variables rather than prescriptions for any specific case.
Sterile technique and perioperative infection prevention are standard intraoperative priorities across procedure types. Use of prophylactic antibiotics, skin preparation protocols, and sterile draping are common elements intended to reduce infectious complications, with specific practices varying by institution and procedure. Hemostasis and minimising tissue trauma may be emphasised to support wound healing. When implants or foreign materials are used, surgeons may discuss material selection and placement options as factors that can affect both early and late outcomes; these are technical considerations rather than endorsements of specific products.
Anesthesia type and intraoperative analgesia are additional considerations that may affect immediate recovery. Local anesthesia with sedation may be appropriate for some procedures and typically allows faster discharge, whereas general anesthesia is used for more extensive operations and may require longer postoperative monitoring. Pain control strategies, including multimodal analgesia, are commonly applied to manage postoperative discomfort and may influence mobility and early rehabilitation. These choices are usually tailored to the procedure and patient factors and are discussed to inform expectations.
Intraoperative documentation and immediate postoperative planning help establish a baseline for recovery. Photographic records, operative notes describing techniques and materials used, and explicit instructions for early care are routine outputs of the operative episode. These records facilitate continuity of care, guide postoperative assessments, and serve as references if unexpected issues arise. Emphasising documentation and clear handover procedures is a common practice aimed at supporting safe transitions to recovery monitoring rather than guaranteeing specific healing trajectories.
Postoperative care frameworks commonly include wound monitoring, activity guidance, and scheduled follow-up visits to assess healing and identify complications. Early postoperative checks often focus on wound integrity, signs of infection, and pain control, while later visits may evaluate scar maturation and functional recovery. Rehabilitation interventions—such as physical therapy for range of motion or scar management techniques for cutaneous procedures—may be part of the recovery pathway. Clinicians typically describe expected timeframes for milestones in recovery while noting that individual variation is common.

Monitoring for and managing complications is an integral part of postoperative care and generally follows established clinical pathways. Early complications can include bleeding, infection, or wound separation, while later issues may involve contour irregularities, sensory changes, or delayed healing. When complications arise, clinicians typically describe a set of potential responses—such as local wound care, bedside procedures, or further surgical intervention—framed as possible options rather than guaranteed necessities. Clear communication about signs that warrant clinical reassessment is commonly provided to patients as a precautionary measure.
Outcome measurement often combines clinician evaluation with patient-reported outcome measures to capture both technical results and the patient’s perspective on appearance and function. Photographic documentation at specified intervals is a standard method to track changes over time. Validated questionnaires—when available for a given procedure—can provide structured data on satisfaction, symptom burden, and quality of life. These measurement approaches are used to inform ongoing care and to support shared decision-making about potential secondary procedures or rehabilitation strategies.
Long-term follow-up considerations may include monitoring implant integrity, evaluating scar maturation, and assessing functional restoration over months to years. Secondary or revision procedures can be part of long-term care planning when adjustments are needed to address aesthetic or functional concerns. Access to multidisciplinary support services—such as physical therapy, lymphedema management, or psychological support—may assist recovery for some patients. These elements are described as components of comprehensive postoperative care and as considerations that may influence long-term outcomes rather than as guarantees of specific results.