
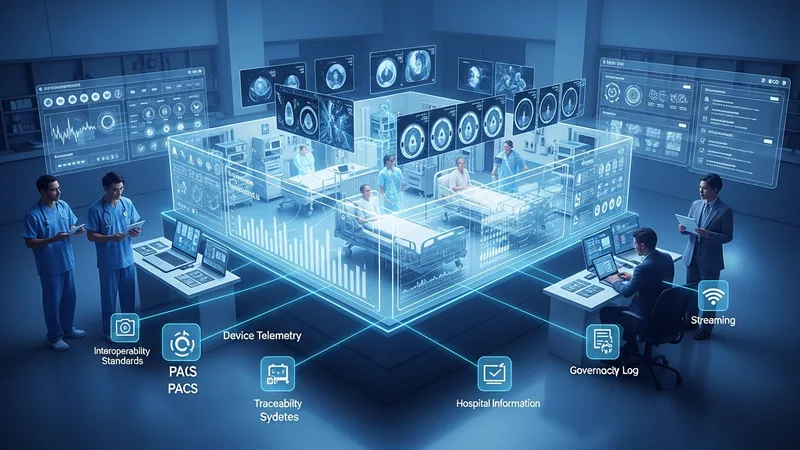
A digital twin in clinical contexts is a computational representation of a real-world healthcare element—such as a medical device, a care pathway, or an aggregated patient data environment—that mirrors state and behavior so that stakeholders can examine scenarios, monitor performance, and explore options without interacting with the physical system. These models combine data streams from electronic health records, imaging, device telemetry, and environmental sensors with simulation algorithms. In practice, the virtual replica may update in near real time and can be used to visualize processes, test configuration changes, or support operational planning within a provider organization.
Implementations typically involve collaboration among clinicians, IT staff, biomedical engineers, and external platform providers. In the United States, projects often connect digital twins to hospital information systems, picture archiving and communication systems, and device management platforms so the virtual model reflects clinical workflows and regulatory requirements. Data harmonization and traceability are frequent priorities, and teams may adopt interoperability standards and defined governance to ensure the twin aligns with clinical and operational objectives without making clinical recommendations directly from the model.
Comparatively, these examples illustrate different technical emphases: cloud-native graph modeling, accelerated medical imaging and AI workloads, and vendor-integrated device and imaging simulations. Selection among such options may depend on whether a provider seeks facility-level operational simulation, patient-specific modeling, or device lifecycle management. Cost structures typically vary by scale and integration needs and may include cloud consumption, software licenses, and engineering services. Teams often evaluate integration overhead, data residency, and compatibility with local electronic health records when determining architecture.
Operationally, providers may use digital twins to examine scheduling, capacity planning, and equipment maintenance scenarios without disrupting care delivery. For instance, a hospital might simulate alternate staffing patterns or imaging workflows to estimate impacts on throughput. These simulations may rely on historical EHR timestamps, operational logs, and device telemetry. When applied cautiously, the process can surface workflow bottlenecks and support planning; outcomes reported in project studies often describe potential efficiencies rather than guaranteed improvements.
From a clinical perspective, patient-specific twins can combine imaging, physiology, and monitored signals to create individualized computational models that support planning or training. Such models often require high-fidelity inputs—imaging resolution, sensor calibration, and validated physiological submodels—to be useful for simulation. In the United States, academic medical centers may publish pilot studies demonstrating feasibility for particular applications, though these studies typically emphasize research contexts and technical validation rather than established clinical practice changes.
Data governance and interoperability are central considerations. Providers commonly adopt standards such as HL7 FHIR to exchange structured clinical data and may use vendor APIs to ingest device telemetry. Privacy protections, de-identification, and role-based access control are typical elements of governance models, especially when research or multi-institutional collaboration is involved. Teams often implement logging and validation routines so that model inputs and outputs remain auditable for operational review and regulatory scrutiny where applicable.
In summary, creating virtual replicas of clinical systems or patient data environments involves technical modeling, multidisciplinary collaboration, and attention to data governance and integration. Implementations in U.S. healthcare settings may draw on cloud platforms, vendor tools, and standards-based interfaces to align virtual models with operational and clinical workflows. The next sections examine practical components and considerations in more detail.

Clinical staff often serve as domain experts who define use cases, validate model behavior, and interpret simulation outputs. In United States health systems, physicians and nurses may participate in requirements workshops and validation studies to confirm that model scenarios reflect realistic patient care pathways. Biomedical engineering and clinical engineering teams typically address integration with medical devices and equipment telemetry, ensuring that device data schemas are captured correctly. These groups may coordinate maintenance and device lifecycle data so the twin can represent performance and failure modes relevant to operational planning and safety review.
Information technology and data teams implement ingestion pipelines, data normalization, and storage strategies. Many U.S. providers operate with commercial electronic health record systems such as Epic or Cerner, and data teams often use vendor-provided interfaces or HL7 FHIR endpoints to feed clinical data into modeling platforms. IT teams also set up cloud or on-premises compute environments, manage identity and access, and coordinate with cybersecurity teams to align the twin’s infrastructure with organizational security policies and incident response plans.
Vendor partners and solution integrators commonly supply modeling engines, platform services, and domain-specific modules. In the U.S., providers may engage established cloud vendors or medical technology companies to supply components; procurement often includes technical statements of work that specify data handling, service levels, and compliance expectations. Contracting teams and legal counsel typically review data use agreements and business associate arrangements under HIPAA when vendors will access protected health information as part of development or operations.
Operational leadership and program managers coordinate project scope, timelines, and stakeholder engagement. They may define success metrics that are measurable and time-bound while avoiding clinical directives based solely on model outputs. In larger U.S. health systems, governance committees can include clinical, technical, legal, and quality representatives to oversee phased rollouts, evaluation plans, and change control processes. These governance bodies often emphasize reproducibility and documentation to support internal review and external audits.
Data integration is a core technical requirement. Providers commonly extract structured records, device telemetry, and imaging data to build input datasets for digital twins. In U.S. settings, electronic health record vendors such as Epic provide APIs and extract methods that teams may use, and interoperability standards like HL7 FHIR are frequently adopted to reduce custom mapping. Teams should consider schema translation, timestamp alignment, and data quality checks so that the model receives coherent, time-synchronized inputs for simulation and analysis.

Compute and storage choices vary across deployments. Cloud platforms that support health-compliant deployments—such as Microsoft Azure with healthcare services—are often used to host modeling engines and scaled compute workloads, including GPU-accelerated processing for imaging or machine learning. On-premises options may be preferred where data residency or latency constraints exist. Providers typically weigh operational costs, security controls, and integration complexity when selecting a deployment model, and budgeting may account for ongoing cloud consumption and engineering maintenance.
Modeling approaches include physics-based simulations, statistical models, and hybrid machine-learning methods. For patient-specific simulations, imaging-derived meshes and physiological parameters may feed finite-element or computational fluid dynamics models; for operational simulations, discrete-event or agent-based models may represent workflows and resource allocation. Validation plans often include retrospective comparisons with historical outcomes or synthetic test cases to establish that model behavior aligns with expected patterns before using outputs in decision support contexts.
Security and identity management are integral to technical design. In U.S. healthcare environments, multi-factor authentication, encryption at rest and in transit, and strict role-based access are common controls. Teams may also implement auditing and provenance tracking to record data sources and model versions, which supports accountability and traceability. These measures are typically framed as considerations to manage risk and maintain compliance with organizational policies and applicable U.S. regulations.
Privacy regulation and protected health information frameworks guide how data is used to build and run virtual models. In the United States, HIPAA sets baseline requirements for handling individually identifiable health data, and business associate agreements are commonly used when vendors process such data. Providers often seek to de-identify datasets for research or cross-institutional collaboration, applying expert determination or safe-harbor methods while documenting processes and residual re-identification risk as part of governance records.
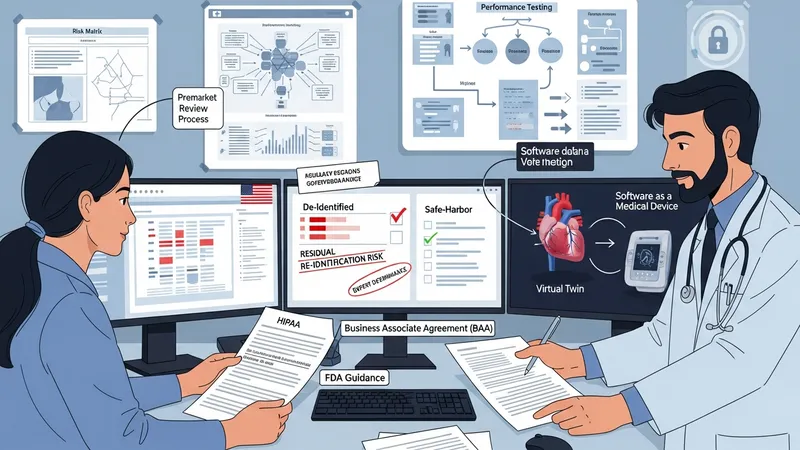
Regulatory oversight can apply when digital twins intersect with device functionality or clinical decision-making. The U.S. Food and Drug Administration (FDA) provides resources addressing digital health and software as a medical device; teams developing models that influence treatment or device operation typically review FDA guidance and engage regulatory affairs to determine whether premarket review or additional validation is needed. Documentation of intended use, risk analysis, and performance testing is typically part of that evaluation.
Institutional review boards and research governance committees may be involved when models use patient data for research or testing. Many U.S. academic centers require IRB review or determination of exemption for projects that analyze patient data or involve model-derived synthetic cohorts. Providers often establish data access committees to review research proposals, ensuring data minimization and adherence to consent terms. Transparent recordkeeping and periodic audits are typical governance activities to maintain compliance and public trust.
Data governance frameworks usually specify stewardship roles, retention policies, and quality metrics. Providers may adopt cataloging tools that record lineage, versioning, and authorized uses for datasets and models. These practices can support reproducibility and accountability, and they are commonly framed as considerations for long-term maintainability and regulatory readiness rather than guaranteed risk elimination.
Providers may apply digital twins to equipment lifecycle and maintenance planning. For example, imaging departments can combine device telemetry with maintenance logs to simulate failure probabilities and schedule preventive actions; such initiatives often report potential improvements in utilization and downtime in pilot studies at U.S. hospitals. Biomedical engineering teams typically collaborate with vendors to validate telemetry interpretation and to ensure that simulated scenarios reflect realistic device behavior and manufacturer guidance.

Simulation of clinical workflows and resource allocation is another common application. Emergency departments and perioperative services may use discrete-event models to test alternative staffing, room assignments, or supply chain arrangements. In the U.S., hospitals that pilot such simulations often pair operational analysts with clinical leads to interpret results and translate findings into process experiments; these pilots usually emphasize measurement and iterative refinement rather than immediate system-wide changes.
Patient-specific modeling for surgical planning or device sizing is emerging in specialized centers. These projects often require high-resolution imaging, multidisciplinary validation, and careful clinical governance. In academic settings, teams may publish feasibility work demonstrating how a virtual model could inform planning; such publications typically note limitations and call for prospective studies before broad clinical adoption. Providers considering similar projects usually plan staged validation and clinician training as part of capability building.
Capability development commonly combines technical hiring, partnerships, and internal training. U.S. providers often form cross-functional teams that include data engineers, clinical informaticists, and simulation specialists. Considerations include establishing reproducible pipelines, documenting model assumptions, and scheduling regular model performance reviews. These practices are typically presented as prudent organizational measures to support the reliable use of virtual models within clinical and operational contexts.