
Selective Estrogen Receptor Degraders (SERDs) represent a class of compounds used in the management of certain forms of breast cancer. These agents function by targeting estrogen receptors within cancer cells, binding to them, and causing their breakdown. This process typically results in decreased estrogen-driven signaling, which can play a role in slowing the proliferation of hormone receptor-positive breast cancer cells. SERDs are often researched and used in clinical settings focused on tailored cancer therapies that address specific biological pathways.
Understanding the functioning of SERDs involves examining how they distinguish themselves from other endocrine therapies. Unlike agents that block estrogen receptors without promoting degradation, SERDs can lead to receptor elimination in addition to inhibition. This mechanism is being studied in various clinical settings to identify patient groups that might benefit most, emphasizing a personalized approach to breast cancer care. Ongoing research continues to clarify how SERDs integrate with other treatment modalities over different stages of disease management.
Fulvestrant is frequently referenced as a standard injectable SERD, typically reserved for postmenopausal individuals with metastatic, hormone receptor-positive breast cancer who have experienced disease progression following endocrine therapy. Its intramuscular administration route requires clinic visits for dosing, with pharmacokinetic and dosing schedules well established in literature. The mechanism of receptor degradation distinguishes its effects compared to antagonists.
Elacestrant, a more recently described oral SERD, is studied for its activity in various advanced breast cancer settings, including against tumors showing resistance to prior endocrine therapies. Its oral administration format may provide additional dosing flexibility compared to injectables, though safety and efficacy profiles remain under continuous clinical investigation to define benefits and tolerability.
Amcenestrant and similar next-generation SERDs are the focus of ongoing clinical trials evaluating their effect on cancers that have developed resistance to earlier therapies. These studies typically assess receptor degradation capabilities, molecular selectivity, and differentiation from other treatment classes. Early clinical findings are used to identify appropriate patient populations for future therapy options.
Clinical use of SERDs is heavily guided by tumor biology, hormone receptor status, and prior treatment exposures. Treatment strategies often account for the specific type of SERD, side effect profiles, route of administration, and integration with combination approaches such as targeted therapy or chemotherapy. Selection is made collaboratively based on clinical trial data, guidelines, and patient-centered considerations.
This introduction outlined the main agents and foundational principles related to SERDs in breast cancer therapy. The next sections examine practical components and considerations in more detail.
SERDs exert their effects primarily by entering breast cancer cells and binding to estrogen receptors with high affinity. Upon attachment, SERDs induce a conformational change that marks the receptor for degradation. The loss of estrogen receptors on the cell surface reduces the cell's responsiveness to estrogen, which can play a significant role in limiting the growth signals that drive certain breast cancers.
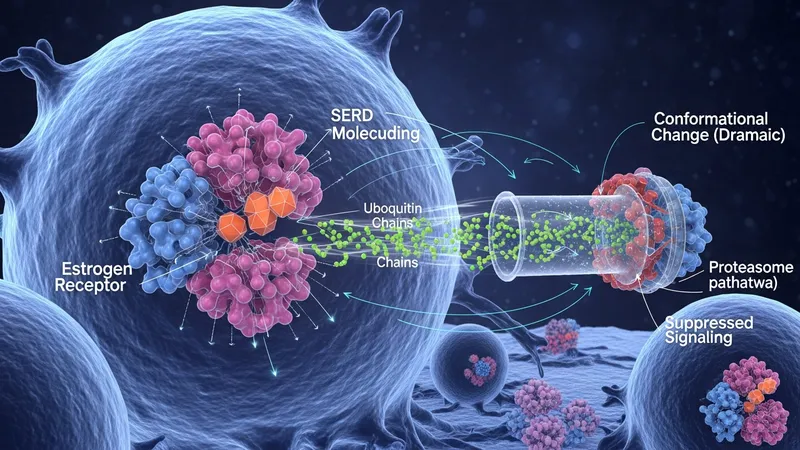
The process of estrogen receptor degradation by SERDs is distinct from simple blockade. While both SERDs and selective estrogen receptor modulators (SERMs) bind to the receptor, only SERDs facilitate its breakdown within cellular proteasome pathways. This dual action—receptor antagonism and facilitated degradation—typically leads to a more complete suppression of estrogen-dependent signaling in cancer cells.
Ongoing laboratory and clinical research continues to assess the potency and selectivity of different SERDs. Individual compounds, such as fulvestrant, have demonstrated ability to eliminate a substantial proportion of estrogen receptors in tumor tissue. This characteristic may enhance their utility in settings where resistance to other forms of endocrine therapy has emerged.
Comparative studies between SERDs and other anti-estrogen therapies reveal that SERDs may reduce the chance for cancer cells to bypass treatment by upregulating estrogen receptor production. As a consequence, they are being studied in various lines of treatment to understand their impact on long-term cancer control within hormone receptor-positive disease.
The clinical application of SERDs is primarily seen in hormone receptor-positive, HER2-negative advanced or metastatic breast cancer. Typically, fulvestrant and similar agents are prescribed for patients who have progressed on previous hormonal therapies. Administration protocols, dosing schedules, and monitoring requirements may vary depending on the specific agent chosen and the patient’s prior treatment experience.

In recent years, the introduction of oral SERDs such as elacestrant has broadened investigational and clinical options. Ongoing trials are assessing whether these agents can serve as alternatives to injectable therapies, particularly in cases where intravenous or intramuscular administration presents challenges for chronic care.
Clinical guidelines and decision-making algorithms emphasize individualized therapy planning. Factors such as tumor hormone receptor levels, patient comorbidities, previous responses to endocrine agents, and potential for drug resistance are commonly considered. The multidisciplinary nature of cancer care means oncologists, pharmacists, and patients work together to determine when a SERD fits into a treatment plan.
Many SERDs are also evaluated in combination strategies, including concurrent use with cyclin-dependent kinase 4/6 (CDK4/6) inhibitors or mTOR inhibitors. These combination approaches are designed to target multiple pathways influencing tumor growth and have formed the basis for several active clinical trials.
One key challenge in SERD therapy involves management of side effects, which may include injection site discomfort, fatigue, and gastrointestinal disturbances, depending on the agent and route of administration. Patients receiving injectable SERDs may require in-clinic visits, while oral agents could change monitoring patterns but bring their own unique side effect profiles.

Drug resistance represents another important consideration. Some cancer cells may adapt to endocrine therapy by mutating the estrogen receptor or activating alternative growth pathways. Research into next-generation SERDs such as amcenestrant aims to address these challenges by retaining efficacy in tumors with certain resistance features.
Access to SERDs can be influenced by regulatory approval status, reimbursement policies, and availability of clinical trials. Patients and providers may consider these factors alongside the scientific rationale for choosing one agent over another. Health care systems strive to balance innovation with prudent adoption of new agents based on evolving evidence.
Investigators continue to refine biomarker testing and molecular diagnostics to identify individuals most likely to benefit from SERDs. This personalized strategy may help minimize exposure to ineffective treatments and guide the development of new agents with improved activity in specific tumor subtypes or stages.
The area of SERD development is marked by the emergence of novel molecules designed to improve receptor degradation efficiency and bioavailability. Many new oral agents, such as elacestrant, are being studied for their potential to address unmet needs in hormone receptor-positive breast cancer with manageable side effect profiles and expanded patient selection.

Clinical trial networks are investigating the role of SERDs as first-line, second-line, and combination therapies. Adaptive trial designs may help define which cancer subtypes, prior exposure histories, and molecular alterations are associated with optimal benefit from SERD treatment. Real-world data are also being collected to validate findings from highly controlled research settings.
Translational science in this area includes exploration of cancer cell molecular signaling, mechanisms underlying acquired resistance, and possible biomarkers of response. Success in these fields may provide more precise matching of agents with individual patient or tumor characteristics over the coming years.
Ongoing collaboration among scientists, clinicians, and regulatory agencies aim to bring new SERD treatments from research environments into routine therapeutic options for breast cancer care. While continued research is necessary, the role of SERDs in managing estrogen-driven cancers is likely to expand as knowledge advances and additional agents become available.