
The concept addressed here is the role of a newer class of medicines that act on gut-derived hormone pathways to influence body weight in individuals with chronic excess weight. These agents interact with receptors involved in appetite regulation, glucose handling, and energy balance. One medication in this class is designed to engage more than one incretin pathway concurrently, which may alter hunger signals and metabolic responses when used under clinical supervision as part of a broader care plan for weight management.
Within this pharmacologic approach, clinicians and researchers consider how a drug’s mechanism, dosing regimen, and safety profile align with patient needs. Use of such medicines typically occurs alongside behavioral and nutritional strategies rather than as a solitary measure. Decision-making often reflects clinical trial data, regulatory indications, individual health status, and monitoring requirements. Framing these options neutrally helps readers understand where this pharmacologic strategy fits within the broader landscape of chronic weight management.

Mechanistically, agents that target incretin pathways may affect several physiologic processes relevant to body weight. These processes can include altered gastric emptying, reduced appetite sensations, and changes in energy intake. The degree and pattern of these physiologic effects depend on receptor specificity, dosing, and individual variability. Researchers often evaluate pharmacologic impact using endpoints such as changes in body weight, metabolic markers, and patient-reported appetite measures. Interpretation of results typically accounts for trial design, comparator groups, and duration of follow-up rather than assuming uniform outcomes across populations.
Clinical trial contexts for these medicines often involve randomized, controlled designs that compare a study drug to placebo or an active comparator, together with standardized lifestyle guidance. Reported outcomes in published trials may include average changes in body weight, proportions of participants reaching specified thresholds of weight loss, and secondary metabolic outcomes. Safety monitoring is an integral part of trials, with gastrointestinal effects and other adverse events documented systematically. Regulatory approvals in different jurisdictions are based on assessments of benefit relative to known risks within the trial populations studied.
When considering use in routine care, clinicians and patients typically weigh potential benefits, tolerability, contraindications, and monitoring logistics. Common clinical considerations include baseline assessments of medical history, concomitant medications, and screening for conditions that could interact with therapy. Follow-up schedules are typically set to assess efficacy signals, side effect profiles, and dose adjustments. Access and affordability may influence treatment planning since coverage and pricing structures vary across health systems and insurers.
Comparative considerations between dual-acting agents and GLP-1–selective agents often focus on mechanism differences, dosing cadence, and observed tolerability patterns in trials. Dual-acting molecules engage more than one incretin receptor, which can theoretically produce distinct metabolic effects compared with single-receptor agents; however, the clinical relevance of those differences is evaluated in head-to-head studies and meta-analyses. Clinicians commonly interpret comparative data with caution, emphasizing that population averages may not predict any one person’s response. Shared decision-making frameworks often accompany discussions when multiple pharmacologic choices are available.
In summary, medications that influence incretin-related pathways represent one component of chronic weight management strategies. Their mechanisms, trial evidence, safety considerations, and integration with lifestyle measures are central to understanding how they may fit into care plans. The next sections examine practical components and considerations in more detail.
Agents that engage incretin receptors typically act through several physiologic pathways relevant to appetite and metabolism. A dual GIP/GLP-1 agonist can interact with receptors in the gut, pancreas, and central nervous system, which may modulate insulin secretion, appetite signaling, and gastrointestinal motility. These combined effects often manifest as changes in caloric intake and glycemic markers in clinical studies. Researchers emphasize that individual variability in receptor expression and metabolic state can influence response magnitude. Understanding mechanistic pathways helps clinicians and investigators interpret trial outcomes and consider likely effects in diverse clinical scenarios.
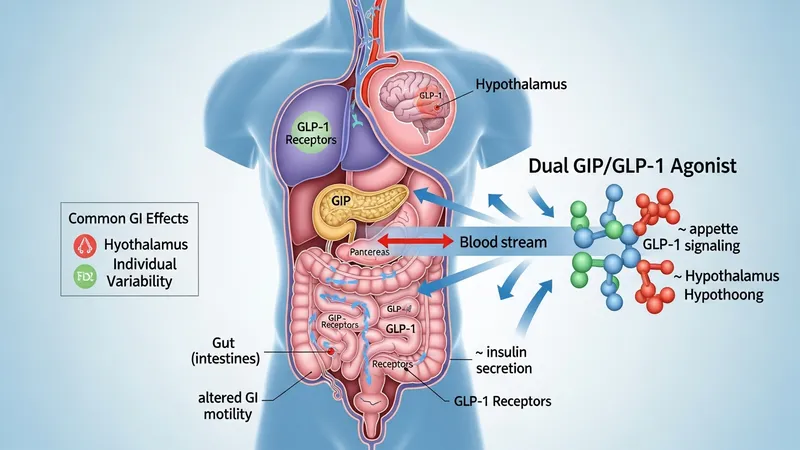
Gastrointestinal responses are commonly observed when initiating incretin-based therapies and can include nausea, early satiety, and changes in bowel habits. Such effects are often dose-related and may attenuate over time for some individuals. Monitoring protocols in clinical practice and research commonly include progressive titration regimens to balance onset of action with tolerability. Pharmacokinetic properties—such as half-life and route of administration—also shape dosing frequency and patient experience. These pharmacologic attributes are part of pragmatic discussions about integrating medication into longer-term weight management plans.
Metabolic consequences beyond weight change are often secondary endpoints in clinical studies. Investigators typically evaluate fasting glucose, hemoglobin A1c, lipid profiles, and blood pressure among other markers. Some agents were initially developed to address glycemic control in people with type 2 diabetes and later studied for effects on body weight. When interpreting metabolic endpoints, it is important to note that population-level trends in trials may not translate directly to individual outcomes and that concurrent lifestyle modifications commonly contribute to observed changes in metabolic markers.
Preclinical and clinical pharmacology research continues to refine understanding of receptor-specific effects and downstream signaling. Ongoing studies explore dose–response relationships, long-term safety, and mechanisms of weight regain after discontinuation. Scientists and clinicians often recommend that mechanistic insights be integrated with clinical data to form balanced expectations about likely benefits and limitations. These considerations may inform monitoring strategies and collaborative decision processes between clinicians and patients considering such medicines.
Randomized controlled trials have been the primary evidence base for evaluating these therapies’ effects on body weight and related metabolic outcomes. Trials often include standardized lifestyle advice for all participants and vary in duration from months to multiple years. Reported outcomes typically emphasize mean changes in body weight versus comparator groups, proportions achieving defined weight-loss thresholds, and safety endpoints. Systematic reviews and meta-analyses synthesize these trials to assess consistency of effects across study populations, though heterogeneity in design and participant characteristics is common and often discussed in interpretive summaries.
Interpretation of trial data frequently considers population selection criteria, such as baseline body mass index ranges, presence of comorbid conditions, and prior treatment histories. Many trials enroll adults with established criteria for chronic weight management, and exclusion criteria commonly omit individuals with certain medical conditions or prior surgical procedures. These inclusion and exclusion patterns can limit generalizability, so clinicians and researchers typically view trial findings as informative but not universally predictive for all patients. Reporting standards in trials aim to clarify these contextual factors.
Endpoint selection in studies includes both objective measures and patient-centered outcomes. Objective endpoints include absolute and relative weight change and metabolic laboratory markers; patient-centered outcomes may cover quality of life, physical function, and treatment satisfaction. Safety reporting documents adverse events comprehensively, with attention to events that are likely to be drug-related. Regulatory reviews assess both efficacy and safety data collectively, and labeling reflects populations and outcomes supported by evidence rather than broader claims beyond trial scope.
Long-term extension studies and post-marketing surveillance provide additional data on durability of effect and rare adverse events. These sources often help to clarify whether initial trial results persist, attenuate, or change over longer follow-up. Observational cohorts and registries can supplement randomized data but are interpreted with caution because of potential confounding. Stakeholders typically use the full spectrum of evidence to form balanced perspectives on how these therapies may contribute to chronic weight management strategies.
Safety profiles for incretin-targeting medications are characterized in clinical trials and post-marketing experience. Commonly reported tolerability issues include gastrointestinal symptoms such as nausea and transient digestive changes; these are frequently dose-related and may lessen with gradual dose escalation. Clinicians typically recommend baseline assessments for conditions that could influence safety, such as pancreatitis history or specific gastrointestinal disorders, and monitor for adverse events during follow-up. Risk communication is framed around probabilities and the need for individualized assessment rather than categorical assurances.

Laboratory monitoring is often part of clinical protocols for these agents. Monitoring may include metabolic panels, assessment of glycemic markers when relevant, and periodic reviews of renal and hepatic function depending on comorbidities and concomitant medications. Medication interactions and effects on absorption of other oral therapies can be a consideration, and prescribers commonly review concurrent treatments to minimize interaction risks. Shared decision-making discussions emphasize trade-offs and the need for ongoing monitoring rather than prescriptive assertions about outcomes.
Patient-reported experiences and adherence patterns influence tolerability assessments in practice. Some individuals may adjust to side effects within weeks, while others may require dose adjustment or discontinuation. Clinicians often document symptom trajectories and use standardized adverse event reporting tools in research settings. Education about expected time courses and common side effects—presented in neutral, factual language—can help align expectations without suggesting guaranteed tolerability. Professional societies frequently publish guidance on monitoring that frames considerations rather than directives.
Special populations, such as people with certain chronic conditions or those who are pregnant or breastfeeding, are often excluded from initial trials, which leads to limited direct evidence in these groups. Regulatory labels and clinical guidance typically specify populations studied and known limitations. When evidence gaps exist, clinicians and researchers rely on registries, observational data, and expert consensus to inform discussions, emphasizing uncertainty and the need for individualized clinical judgment based on available evidence.
Access to these medications often depends on regulatory approvals, payer coverage, and clinical guidelines in a given healthcare system. Cost implications can vary substantially across regions and insurance arrangements; patients and clinicians commonly encounter variable coverage policies that influence out-of-pocket expense. Health systems and insurers typically consider indications supported by clinical data when formulating coverage criteria. Understanding reimbursement pathways and documentation requirements for chronic weight management therapies can be an important part of practical planning.

Practical integration into care pathways often involves multidisciplinary coordination, including primary care providers, endocrinologists, dietitians, and behavioral health professionals. Structured follow-up schedules that assess efficacy, tolerability, and adherence are commonly recommended in clinical programs. Educational materials that describe expected timelines for physiologic changes and common side effects may be provided so patients have realistic expectations. Care teams typically treat pharmacotherapy as one component among behavioral, nutritional, and physical activity strategies within comprehensive management plans.
Cost-management strategies that are discussed in non-promotional contexts include reviewing insurance formularies, prior authorization processes, and available patient assistance programs where relevant. Healthcare providers may document clinical rationale and previous treatment attempts to support coverage requests, and many systems maintain pathways for medication initiation and monitoring. These administrative aspects are practical considerations that can affect whether and how a medication is implemented as part of long-term care.
Ongoing research into real-world effectiveness, long-term outcomes, and cost-effectiveness continues to inform how these medicines are positioned in clinical practice. Stakeholders often evaluate evidence from clinical trials alongside observational data and economic analyses to form balanced policies. Readers interested in implementation details typically consult clinical guidelines and payer resources for up-to-date, jurisdiction-specific information rather than relying on general statements about availability or cost.